
Untuk versi Bahasa Indonesia, silakan kunjungi tautan ini: link
Weekly Findings Report
Week 1, 23-24 April 2020
Snapshot of Findings
- Cases (23 April 2020): In Bone 17,145 people tested; 0 infections; 9 under treatment (PDP); 7,645 under surveillance (ODP); and 282 at risk (ODR) Source: Gugus Tugas
- Survey total of 89 participants, data collected in Bone from 23-24 April 2020.
- Health behaviors. Use of face masks was high, with 74.2% using fabric face masks (non medical), 19.1% using medical masks. Hand washing with soap after doing activities outside was also high (85.4%).
- Social distancing. 97.7% reported going out at least 1-2 times a week, 2.2% did not go out at all. 57.3% went out 1-2 times a week, 24.7% went out every day. 47.2% asked other people to stay at least 1 meter away; 42.7% kept a distance of 1 meter from other people.
- Economic impacts. 51.7% reported income has decreased; 42.7% had difficulty meeting daily needs, and 7.9% lost their jobs.
- Social and personal impacts: 62.9% feared infection by/of other people; 31.5% felt stressed or angry, 15.7% reported being afraid of isolation (in treatment).
- Communication channels. Information on COVID-19 from television was high (85.4%) and considered the most reliable channel (71.9%). The most reliable source of COVID-19 information was the national government (64.0%).
- Social support received. 76.4% received no support, 15.7% received government help; 6.7% from community organizations (e.g., RT, RW, PKK) and 1.1% from NGOs.
- Social support given. 12.4% fundraised; 16.9% distributed donations; 13.5% (n-12) donated to community organizations; 15.7% became volunteers.
- Information still needed. 25.8% said they need information about types of face masks; 51.7% (n=46) wanted available health services.
1. Background
Coronavirus disease 2019 (COVID-19) is a virus first identified in Wuhan, China and reported to the WHO in December 2019. In January 2020, the WHO declared COVID-19 a global health emergency. Most people only experience mild respiratory illness symptoms. However, some people can experience severe symptoms, including pneumonia, resulting in lung damage and death (Sani, Mariska, & Prasetya, 2020). COVID-19 is more dangerous for older people and those with pre-existing medical conditions, such as diabetes, high blood pressure and heart disease (Liu et al, 2020). The first case was reported in Indonesia on 2 March 2020 and on 13 April the government declared a national disaster. On 10 April, the government initiated a Large Scale Social Restrictions (PSBB) policy started in Jakarta, including closing schools, workplaces, restricting movement and closing public places. The local, Indonesian and global effects of Covid-19 have an impact on people’s lives, families, communities and economies.
Bone consists of 27 kecamatan (sub-district), 335 desa (villages), with Watampone as the capital. Bone has 751,026 people, the most populous in South Sulawesi Province. Similar to many regions, Bone has engaged in Covid-19 management and prevention. By 23 April 2020, a total of 17,145 people have been tested with zero confirmed cases; 9 patients under treatment (Pasien Dalam Pengawasan/PDP); 7,645 under surveillance (Orang Dalam Pantauan/ODP); and 282 people at risk (Orang Dalam Risiko/ODR) (Task Force of COVID-19 Prevention in Bone). Health promotion efforts conducted by the government include cleaning with disinfectant, distribution of face masks, and hand sanitizer. In 2019, as part of its BERANI program, UNICEF commissioned Tulodo to manage a project in Bone to prevent child marriage and improve menstrual health. The project staff and networks are being used to implement this study.
2. Objectives
This study aims to answer the question: what is the impact of the Covid-19 pandemic in Indonesia over time? It explores how communities have responded, including any changes in health behaviours (e.g., use of face mask, practicing handwashing with soap, and social distancing) and how this outbreak has affected their economic status. We also explore their exposure to communication channels and campaign messages. This study also provides recommendations for partners and stakeholders in Bone to consider.
3. Methodology
This cross-sectional study uses a mix of quantitative and qualitative methods, conducted weekly from 23 April to 15 May 2020. This enables us to track changes from week to week and also over the life of the study. The quantitative survey is conducted via phone and online. We use snowball sampling methods to recruit participants via phone, while for online we distribute it through our partners. The total target sample is 450 respondents. For the qualitative study, we will conduct 15 interviews via phone.
4. Results
Below are the results from the first week of data collection (23-34 April 2020). A total of 89 respondents joined the study (20 via phone and 69 via online). These results are preliminary and subject to change.
4.1 Sample characteristics
- Location. 16.9% (n=15) from Tanete Riattang Barat sub-district, 13.5% (n=12) each from Cina and Salomekko.
- Gender.55.1% female, 44.9% male.
- Age. 36% aged 21-30 years; 20.2% aged 31-40 years, 19.1% aged 41-50 years, 11.2% aged 51-60 years, 9% aged 11-20 years, 3.4% aged 61-70 years, and 1.1% aged above 70 years
- Breadwinner. Father (59.6%), mother (16.9%), other adult males (16.9%), and other adult females (9%).
- Education. 4.5% (n=4) completed elementary school, 6.7% (n=6) junior high school, 19.1% (n=17) senior high school, and 62.9% (n=56) university/college.
- Income. 24.7% (n=22) had permanent jobs, 22.5% (n=20) said crop sales. 28.1% (n=25) received less than Provincial Minimum Wage (UMP). Upah Minimum Provinsi (UMP) in South Sulawesi is IDR 2,860,382 (USD200) per month.
- Government support. 6.7% (n=6) received goods from government agencies, 3.4% (n=3) received cash, 6.7% (n=6) received services, and 80.9% (n=72) received nothing. Of those who received support, 35.3% received Beras Sejahtera (Rastra) rice allowance; 23.5% received Program Keluarga Harapan (PKH) cash payments; 5.9% received support from Kelompok Usaha Bersama (KUBE); 64.7% were registered on the Healthy Indonesia Card (KIS) program; and 5.9% were registered on the Kartu Indonesia Pintar (KIP) program.
- Elderly. 31.4% said there was one elderly person in the household; 18% had two elderly people, and 4.5% said there were three or more.
4.2 Behaviors
- Handwashing practice. 85.4% (n=76) washed their hands after doing activities outside the house, 62.9% (n=56) before/after eating and drinking, 48.3% (n=43) after handling goods from outside, 28.1% (n=25) after sneezing and coughing, 31.5% (n=28) after shaking hands, 37.1% (n=33) after using the toilet, 32.6% (n=29) before/after preparing food, and 2.2% (n=2) before prayer.
- Handwashing tools. 16.9% (n=15) used running water, 93.3% (n=83) running water and soap, 33.7% (n=30) used hand sanitizer, and 9% (n=9) wiped hands using cloth/tissue.
- Face masks. 6.6% (n=6) did not use a face mask, 74.2% (n=66) used fabric face masks (non medical), 19.1% (n=17) using medical masks.
- Social distancing. 47.2% (n=42) asked other people to stay at least 1 meter away; 42.7% (n=38) maintained 1 meter from other people, 23.6% (n=21) asked others to wear a face mask, and only 10.1% (n=9) provided someone with a face mask.
- Outside activities. 57.3% (n=51) reported going out 1-2 times a week, 24.7% (n=22) went out every day, 15.7% (n=154) went out 3-5 times a week, and 2.2% (n=2) did not go out.
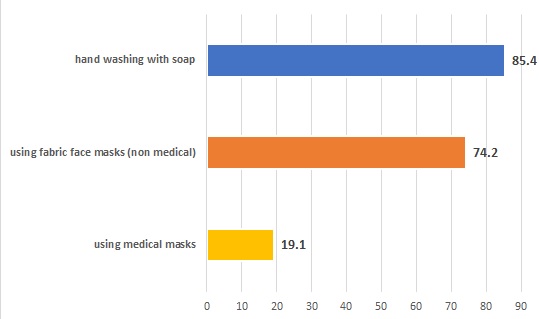
Figure 1. Health behaviors related to COVID-19
4.3 Impact of COVID-19
- Employment. 32.8% (n=29) worked from home, 25.8% (n=23) temporarily did not work, 23.6% (n=21) worked as usual, 18.0% (n=16) worked as usual but with restrictions (example: changes in work schedules / shifts).
- Income. Most respondents (44.9%, n=40) reported income has decreased, 29.3% (n=26) reported no income (IDR 0), and 25.8% (n-23) reported the same income.
- Feeling isolated. 67.4% (n=60) did not feel isolated, 21.3% (n=19) reported sometimes feeling isolated.
- Other impacts. 42.7% reported difficulty meeting daily needs. 51.7% (n=46) reported that their revenue has decreased, 7.9% (n=7) reported losing their jobs, 31.5% felt stressed or angry, 62.9% (n=56) feared infection by/of other people; 15.7% (n=14) were afraid of being isolated (due to infection), 24.7% reported being away from family.

Figure 2. Economic, social and personal impacts of COVID-19 on the community
4.4 Communications
- Exposure to COVID-19 related information. Most respondents (85.4%, n=76) received information from television, 73.0% (n=65) from social media, 52.8% (n=47) from online articles, 33.7% from banners/posters, 31.5% from mosques, 24.7% (n=22) from mobile units, 5.6% (n=5) from radio, 16.9% (n=15) from newspapers, 16.9% (n=15) from SMS, and 15.7% from pamphlets. Of those who mentioned social media, 87.7% (n=57) reported getting information from WhatsApp, 78.5% (n=51) from Facebook, 46.2% (n=30) from Instagram, 55.4% (n=36) from YouTube, whilst 4.6% (n-3) from TikTok.
- Source of information. 79.8% (n=71) said their information was from national government, 79.8% (n=71) from provincial/sub-district government, 48.3% (n=43) from the village government, 37.1% (n=33) from religious leaders, 56.2% (n=50) from family members, 50.6% (n=45) from friends and 25.8% (n=23) from neighbors.
- Most reliable information channels and sources. 71.9% (n=64) said television was the most reliable, whilst 11.2% (n=10) said online articles. The most reliable source was national government (64.0%, n=57) and provincial/district government (14.6%, n=13).
- Information still needed. 25.8% (n=23) said they need information about which types of face masks should be used; 31.5% (n=28) said the virus transmission; 32.6% said the number of cases; 51.7% (n=46) wanted available health services; 18.0% (n=16) said hand washing practice; 37.1% (n=33) on the large-scale social restrictions (PSBB); 31.5% (n=28) on the lockdown areas, 50.6% (n=45) need fact checking of hoaxes and misinformation. Only 14.6% (n=13) need information about making face masks, 24.7% (n=22) on making hand sanitizer; 29.2% about mental health.
4.5 Social support given and received
- Social support received. 76.4% (n=68) never received any support, 15.7% (n=14) received government support; 6.7% (n=6) received community organization help (e.g., RT, RW, PKK) and 1.1% (n=1) received NGO support. Of those who received support, 54.5% (n=12) received face masks, 18.2% (n=4) received hand sanitizers, 13.6% (n=3) said groceries (food), and 36.4% (n=8) received other support (internet, electricity, gas or free water).
- Social support given. 42.7% (n=38) did not contribute to social support, 12.4% (n=11) collected donations or fundraised; 16.9% (n=15) distributed donations to beneficiaries; and 13.5% (n-12) donated to community organizations; 15.7% became volunteers. Of those who gave social support, 44.4% (n=16) distributed masks, 13.9% (n=5) distributed hand sanitizer, 2.8% distributed vitamins and supplements, 30.6% (n=11) distributed groceries (food), 22.2% distributed cash, and 2.8% (n=1) distributed other things (internet, electricity, gas or free water).
5. Recommendations
These are the priority recommendations for stakeholders in Bone to consider:
- Boost core behavior change activities to prevent COVID-19 infection, including wearing masks, social distancing, and washing hands with soap. Emphasis should be placed on staying at home, which can be linked to economic incentives (see #4).
- Additional behaviors to be targeted include how to access health services for treatment; also a practical guide on how to make face masks.
- The marketing mix of activities should be intensified with greater investment in content and channels. Television, including local channels, should be a major part as it is most popular and considered most reliable for information about COVID-19.
- Rapid decreases in income and employment require intensive responses from local government and partners. Responses can be delivered through boosts to existing programs, such as KUBE, PKH, Rastras, KIS etc. Support, including labor intensive projects and microcredit, should be delivered through local community channels, for example PKK, BKMT, farmer and fisher groups.
The second wave of data collection will be conducted from 27-30 April 2020. We will update the report on a weekly basis.
Dowload report: Findings Report Covid19-W1-27April2020
References
Gugus Tugas Penanganan Covid-19. (2020). Update data Penanganan COVID-19 Kabupaten Bone. dated 23 April 2020: https://bone.go.id/2020/04/23/update-data-penanganan-covid-19-kabupaten-bone-kamis-23-april-2020-pukul-20-25-wita/
Liu, K., Chen, Y., Lin, R., & Han, K. (2020). Clinical features of COVID-19 in elderly patients: A comparison with young and middle-aged patients. The Journal of infection, S0163-4453(20)30116-X.
Sani, T.P., Mariska, S,., Prasetya, V.G.(2020), How vulnerable are the elderly to COVID-19? https://alzi.or.id/how-vulnerable-are-the-elderly-to-covid-19/
Published by